Dr. Shekhar Chirmade is Minimally Invasive Spine Surgeon In Nashik. Spine surgery is typically recommended only when a period of nonsurgical treatment. such as medications and physical therapy. has not relieved the painful symptoms, caused by the back problem.
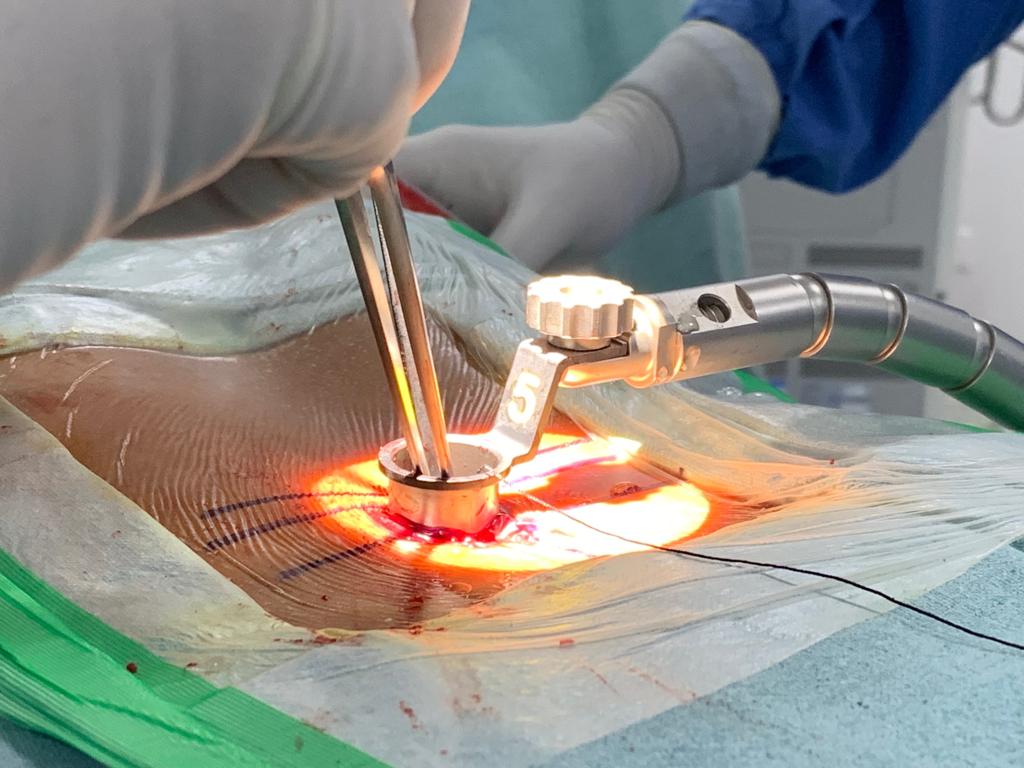
Surgery is only considered if the spine surgeon can pinpoint the exact source of pain, such as a herniated disk or spinal stenosis. Spine Surgery is traditionally done as “open surgery,” meaning the area being operated on is opened with a long incision to allow the surgeon to view and access the anatomy.
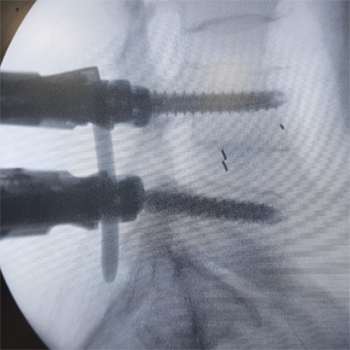
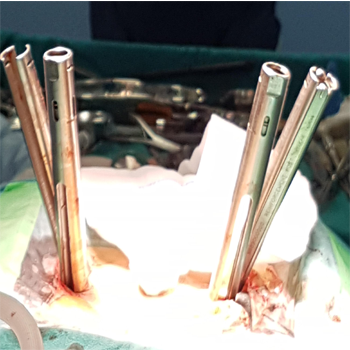
However, technological advances have allowed more back and neck conditions. to be treated with a Minimally Access Surgical Technique (MAST) or Minimally Invasive Spinal Surgery (MISS). Minimally Access Techniques are beginning to be used for a wider range of spine procedures, and have been used for common procedures. like decompression and spinal fusion.
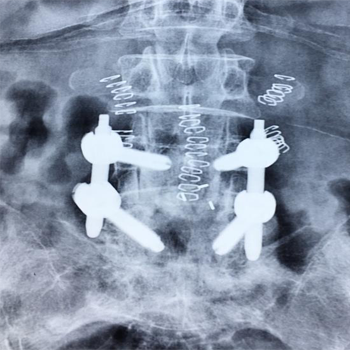
corrects problems with the small bones of the spine (vertebrae). The basic idea is to fuse together the painful vertebrae so that they heal into a single. solid bone As opposed to open spine surgery, Minimally Invasive Surgical approaches can be faster, safer and require less recovery time.