The typical or “classic” form of the disorder (called “Type 1” or TN1) causes extreme, sporadic, sudden burning or shock-like facial pain that lasts anywhere from a few seconds to as long as two minutes per episode.
These attacks can occur in quick succession, in volleys lasting as long as two hours. The “atypical” form of the disorder (called “Type 2” or TN2), is characterized by constant aching, burning, stabbing pain of somewhat lower intensity than Type 1.It is said to be the most excruciatingly painful human condition in the world. TNA’s origin is unknown, but it is often attributed to abnormal blood vessels that compress the nerve, multiple sclerosis, or tumors.
TN is often misdiagnosed as a toothache or TMJ and often they undergo multiple dental procedure or teeth removal.
TN disorders are considered impairments, which can limit an individual’s ability to function on the job.
Pain typically runs in cycles, and it is common for individuals with TN to experience periods of remission. Remission can last for weeks, months, and even years.
Over time, the attacks tend to worsen with fewer and shorter pain-free periods.
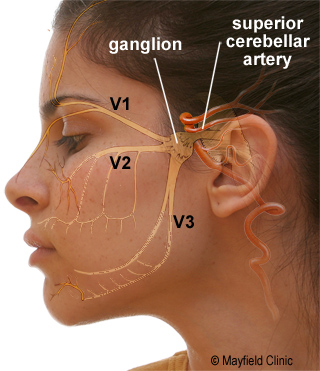
TN is often caused by loss of or damage to the nerve’s protective coating, myelin. Myelin damage results from irritation of the nerve, usually a blood vessel that causes the nerve to be compressed.
TN diagnosis is based primarily on the person’s history and description of symptoms, along with results from physical and neurological examinations.
To rule out other sources of facial pain, doctors typically order a magnetic resonance imaging (MRI) scan. Compression of the nerve by a vessel can sometimes be seen on a MRI.
It is normally treated with anticonvulsants. Tegretol (carbamazepine) is often the most effective treatment. If these medications become ineffective or the side-effects become intolerable, surgical treatment may be offered.
Microvascular Decompression Surgery (MVD): This procedure removes the cause of the TN pain. The MVD offers the best chance of long-term relief without damaging the nerve.
This is an open surgical approach where a small incision is made behind the ear, a small hole is drilled in the skull, and, under microscopic visualization, the trigeminal nerve is exposed.
In most cases, there is a blood vessel (typically an artery, but sometimes a vein) compressing the trigeminal nerve. By moving this blood vessel away from the nerve and interposing a padding made of Teflon felt, the pain is nearly always relieved.
Overall recovery from surgery occurs within 7 days and patient can resume his work on 10th day.
Damaging the nerve: Several procedures can be done to stop the transmission of pain signals to the brain. These procedures actually cause damage to the nerve and relief is obtained. Pain relief do not last for long time and recurrence is very common and often patient has to undergo surgery.
In this procedures needle is passed through cheek in to the nerve and glycerol injections, balloon compression or radiofrequency lesioning is done.